
Drug-Induced Death Prosecutions in New Jersey: When Enforcement Undermines Public Health

By Nikki Tierney, JD, LPC, LCADC, CPRS
NCAAR Policy Analyst
March 2026
Introduction
 Nearly two decades into the nation’s drug crisis, drug-related deaths in the United States remain alarmingly high. The emergency has not plateaued, it has intensified, driven increasingly by a volatile and fentanyl analogue-contaminated drug supply. This is not for lack of evidence about how to reduce mortality or treat substance use disorders. Public health consensus is clear: deaths decline when naloxone is widely available, when access to evidence-based treatment, including medications for opioid use disorder (MOUD) such as buprenorphine and methadone, (which reduce overdose risk by an estimated 50–80 percent)1 is expanded and sustained, and when stigma is reduced rather than reinforced through policy. The tools to save lives exist. The question is whether our legal frameworks reinforce them, or undermine them.
Nearly two decades into the nation’s drug crisis, drug-related deaths in the United States remain alarmingly high. The emergency has not plateaued, it has intensified, driven increasingly by a volatile and fentanyl analogue-contaminated drug supply. This is not for lack of evidence about how to reduce mortality or treat substance use disorders. Public health consensus is clear: deaths decline when naloxone is widely available, when access to evidence-based treatment, including medications for opioid use disorder (MOUD) such as buprenorphine and methadone, (which reduce overdose risk by an estimated 50–80 percent)1 is expanded and sustained, and when stigma is reduced rather than reinforced through policy. The tools to save lives exist. The question is whether our legal frameworks reinforce them, or undermine them.
Even as evidence supports treatment and harm reduction, governments have increasingly revived drug-induced homicide (“DIH”) statutes; punitive measures rooted in a deterrence model that has not demonstrated success in preventing overdose deaths. Originally enacted to dismantle high-level trafficking networks and target so-called “kingpins,” these laws are now frequently imposed in a very different context. Research shows that many prosecutions involve friends, intimate partners, family members, or other co-users, often individuals with substance use disorders themselves, rather than large-scale commercial distributors. In communities already burdened by concentrated poverty and racial disparities in the criminal legal system, enforcement has fallen disproportionately on the most marginalized populations.
Good Samaritan laws are state-level policies meant to provide immunity from arrest or prosecution for possession of a controlled substance and drug paraphernalia for those who call for emergency medical assistance when witnessing an overdose. However, when overdose scenes are treated as potential homicide investigations, the possession-level immunity offered by Good Samaritan laws provides limited reassurance. The person most likely to call for help is often the person most legally exposed. Scholarship consistently finds that fear of arrest or prosecution can deter emergency calls, undermining the very purpose of Good Samaritan protections. In an emergency measured in minutes, perceived legal risk alters behavior; and altered behavior can cost lives.
If drug-related death is a public health emergency, policy must be evaluated by whether it increases the likelihood that someone calls for help, and whether it prevents the next fatality, not solely by the severity of punishment imposed after one has occurred.
Origins, Expansion, and Structure of Drug-Induced Homicide Laws
New Jersey’s strict liability drug-induced death statute, N.J.S.A. 2C:35-9, was enacted as part of the Comprehensive Drug Reform Act of 1987 during the height of the War on Drugs. Under this statute, first degree criminal liability attaches whenever the distribution of a controlled dangerous substance results in a fatality, regardless of motive or commercial gain (N.J.S.A. 2C:35-9). The statute does not require proof of intent to cause death. It does not require proof of profit. It does not require proof of participation in a large-scale trafficking enterprise. The mere provision of drugs, whether for sale or social sharing, is sufficient to establish “distribution.” Because the offense is classified as a first-degree crime (the most serious in New Jersey), it imposes a sentencing range of 10 to 20 years in prison (N.J.S.A. 2C:35-9).
The statute emerged from a broader supply-side enforcement philosophy characteristic of the War on Drugs era. In the 1980s, lawmakers responded to rising drug use, overdose deaths, and crime by escalating penalties aimed at disrupting distribution networks and incapacitating suppliers (Beletsky, 2019; Stepp, 2024)2. At the federal level, the Anti-Drug Abuse Act of 1986 included a drug-induced homicide provision carrying a mandatory minimum sentence of twenty years (Beletsky, 2019). Legislative findings in New Jersey similarly emphasized that the fight against illegal drugs “must be waged aggressively at every level along the drug distribution chain,” with enhanced punishment directed toward “upper echelon drug distributors and kingpins” (N.J.S.A. 2C:35-1.1).
Although New Jersey’s statute was enacted in this earlier enforcement era, its modern use must be understood within a broader national resurgence of DIH prosecutions.
FIGURE 2. ACCUSED-DECEASED DYADS IN DRUG-INDUCED HOMICIDE CASES BY RELATIONSHIP (N=213) (ONLINE NEWS REPORTS 2000-2017)
Beletsky, L. (2019). Utah Law Review “America’s Favorite Antidote: Drug-Induced Homicide in the Age of the Overdose Crisis.“
DIH laws originated during the War on Drugs and remained relatively dormant for decades (Stepp, 2024). In recent years, however, the opioid crisis has driven legislatures to introduce and expand these statutes, and prosecutors have increasingly relied upon them (Stepp, 2024; Beletsky, 2019).
As of the end of 2022, thirty states have enacted DIH laws capable of charging offenses ranging from felonies to murder, with nine states introducing new or expanded legislation in 2021 and 2022 alone (Stepp, 2024). Prosecutions have risen sharply: the number of DIH charges filed in 2018 was more than fifteen times higher than in 2008 (Stepp, 2024). Three states in the Northeast, New York, New Jersey, and Pennsylvania, are among those where such prosecutions are increasing most rapidly (Stepp, 2024).
Importantly, national data indicate that these prosecutions frequently reach beyond large-scale commercial traffickers. Approximately half of DIH cases involve individuals characterized as caretakers, family members, friends, or intimate partners rather than traditional dealers (Stepp, 2024; Miller, 2021)3. In practice, prosecutors often charge the last person who handled the drugs prior to the death, even when that individual shared drugs within a social-use context rather than operating a profit-driven enterprise (Miller, 2021). Such applications of DIH statutes raise serious concerns about the consequences for co-users across the country (Miller, 2021).
State statutory approaches vary considerably. Arizona, for example, limits first-degree murder liability to deaths resulting from the manufacture or transportation of drugs, rather than mere possession or social sharing (Ariz. Rev. Stat. Ann. § 13-1105; Stepp, 2024). Colorado and Wyoming restrict application of their DIH laws to cases involving victims under eighteen (Stepp, 2024). Only four states, Delaware, Mississippi, Rhode Island, and Vermont, provide affirmative defenses when an accused made a good faith effort to seek emergency assistance during an overdose (Stepp, 2024). Against this national backdrop, New Jersey’s statutory structure stands out for what it does not contain.
New Jersey’s statute contains no such limiting language. As explained above, it imposes strict liability based on causation alone, without requiring proof of intent, profit motive, or limitation to large-scale trafficking activity. Although enacted within a policy environment focused on dismantling organized narcotics operations, its reach is defined by outcome alone rather than hierarchy, scale, or demonstrated culpability within a trafficking network.
Beletsky, L. (2019). Utah Law Review “America’s Favorite Antidote: Drug-Induced Homicide in the Age of the Overdose Crisis.“
The NJ Overdose Prevention Act and Emerging Policy Tension
 In 2013, New Jersey began formalizing a harm reduction approach through the enactment of the Overdose Prevention Act, which established Good Samaritan protections intended to reduce legal fear during overdose emergencies. Under N.J.S.A. 2C:35-30, a person who, in good faith, seeks medical assistance for themselves or someone experiencing an overdose may not be arrested, charged, prosecuted, or convicted for low-level possession-related offenses when the evidence was obtained as a result of seeking help. Implementation guidance from the Office of the Attorney General emphasized uniform statewide application so that people in crisis could rely on these protections across jurisdictions4
In 2013, New Jersey began formalizing a harm reduction approach through the enactment of the Overdose Prevention Act, which established Good Samaritan protections intended to reduce legal fear during overdose emergencies. Under N.J.S.A. 2C:35-30, a person who, in good faith, seeks medical assistance for themselves or someone experiencing an overdose may not be arrested, charged, prosecuted, or convicted for low-level possession-related offenses when the evidence was obtained as a result of seeking help. Implementation guidance from the Office of the Attorney General emphasized uniform statewide application so that people in crisis could rely on these protections across jurisdictions4
New Jersey’s overdose policy has evolved alongside a punitive enforcement framework pointing in the opposite direction. Even as the state codified immunity designed to encourage emergency calls, it retained, and increasingly used, its strict liability drug-induced death statute, which imposes homicide-level liability without requiring proof of intent to cause death5. This is not a theoretical contradiction. While national DIH statutes are routinely justified as tools to target “kingpins” and high-level traffickers, research indicates that prosecutions frequently reach friends, partners, and co-users within social networks; often the last person known to have handled or shared the drugs before the fatal event (Miller, 2021; Stepp, 2024). Beletsky (2019) argues that this punitive turn is fundamentally misaligned with overdose prevention: criminalization strategies can deter help-seeking, deepen stigma, and shift overdose response away from a medical emergency framework.
The resulting behavioral incentives are not subtle. Good Samaritan protections rest on a simple premise: people will call 911 if they believe seeking help will not expose them to punishment. But when an overdose scene can also become the starting point of a homicide investigation, possession-level immunity may offer little reassurance. Empirical legal scholarship warns that fear of arrest or prosecution can discourage emergency calls; exactly what Good Samaritan laws are meant to prevent (Phillips, 2020; Carroll et al., 2021)6. Fear of police contact and legal repercussions is repeatedly identified as a leading barrier to seeking emergency assistance during overdoses (Beletsky, 2019). High-profile prosecutions tied to overdose events may intensify those fears by signaling that involvement at the scene, even to save a life, carries serious legal exposure. In this context, partial legal reforms may fail to change behavior when broader criminalization remains intact7. Because only a small subset of jurisdictions provide explicit statutory protections or affirmative defenses shielding Good Samaritans from DIH exposure, and New Jersey is not among them, the chilling effect is difficult to dismiss (Stepp, 2024).
Public messaging may further compound this tension. DIH charges are commonly announced through press releases and media coverage, amplifying the visibility of enforcement. By contrast, sustained, high-saturation public education regarding the scope and limits of Good Samaritan protections is less visible, even though increased awareness increases the likelihood of seeking help. A Washington State evaluation found that individuals who learned about Good Samaritan law protections reported increased willingness to call 911 in future overdose emergencies8. A New York–based study of overdose witnesses found that individuals with accurate, up-to-date knowledge of their state’s 911 Good Samaritan law were more than three times as likely to call 911 during an overdose event compared to those with incorrect knowledge of the law9.
Media reporting functions as a public signal of enforcement priorities. Prominent coverage of homicide prosecutions communicates that legal exposure is severe and immediate, while Good Samaritan protections often receive limited public education and remain poorly understood (Beletsky, 2019).When enforcement messaging dominates public discourse, it shapes perceptions of legal risk at precisely the moment a bystander must decide whether to call for help; and that perceptual difference can determine survival.
Phillips, K. S. (2020). Duke Law Journal “The Incompatibility of DIH Statutes with Due Process.“
Enforcement Expansion and New Jersey Patterns
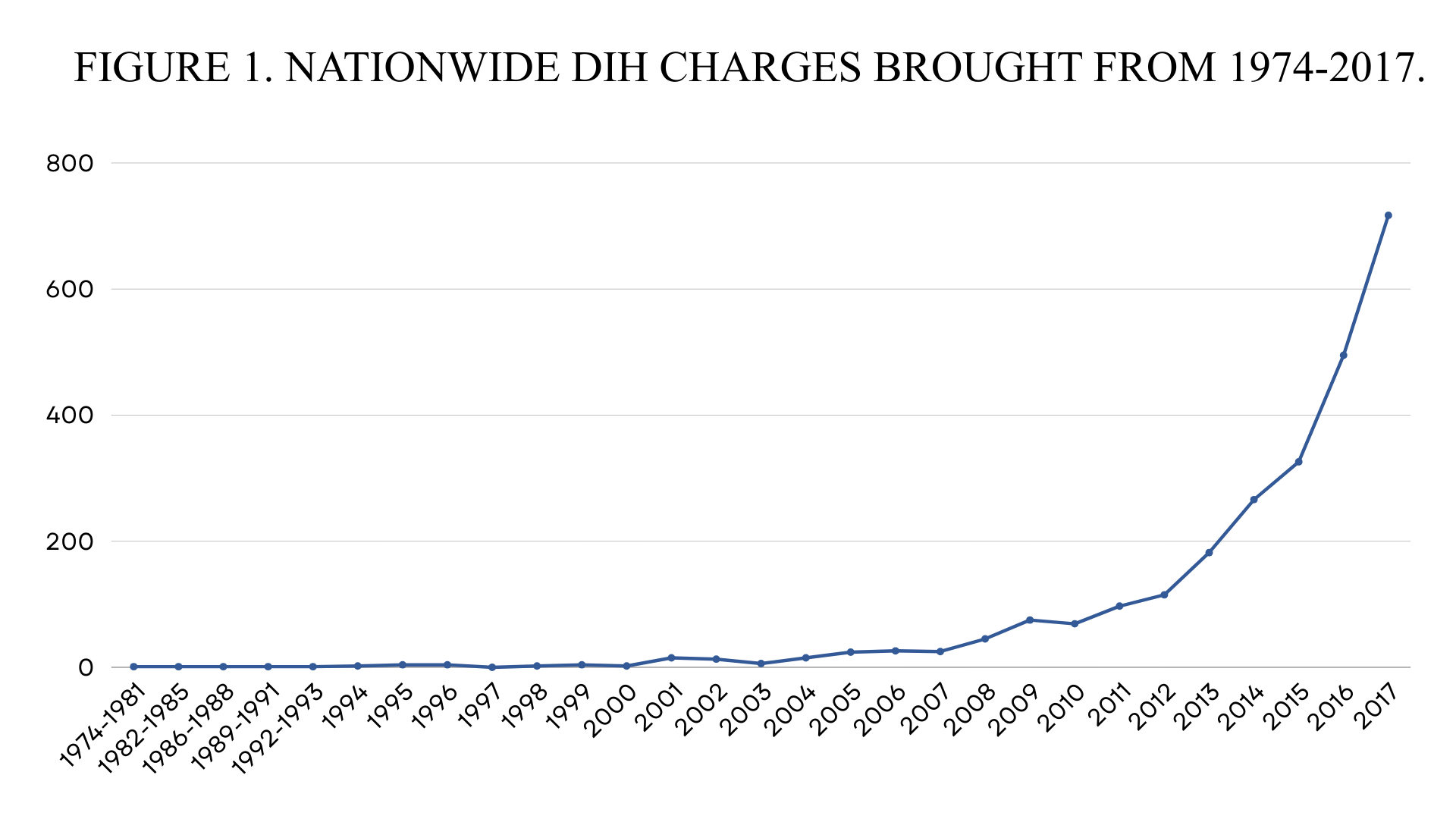
DIH prosecutions have increased sharply nationwide over the past decade, reflecting a revival of War-on-Drugs-era legal tools in the opioid era (Beletsky, 2019; Stepp, 2024). Analyses using media-trend data as a proxy for prosecution activity indicate that news reports of DIH charges rose from 43 mentions in 2008 to 686 in 2018 (Stepp, 2024). Data summarized in the Duke Law Journal similarly show media reports increasing from 363 in 2011 to 1,178 in 2016, an increase of more than 300% in five years (Phillips, 2020). An estimated 2,534 DIH prosecutions occurred between 1975 and 2017, with nearly 80% taking place after 2013 (Carroll et al., 2021).
This expansion reflects more than statutory availability. Prosecutorial networks have actively disseminated strategies for investigating overdose death scenes and building DIH cases, including formal training initiatives (Beletsky, 2019). The surge therefore represents a deliberate institutional strategy rather than passive enforcement.
This broader national expansion provides important context for understanding the state-level enforcement patterns that have emerged in recent years, although the rise has not been evenly distributed. Roughly half of reported charges in one dataset came from Ohio, Illinois, Wisconsin, and Minnesota, while states including New York, New Jersey, and Pennsylvania have been identified as among the fastest-rising jurisdictions (Stepp, 2024). Prosecutorial theories often focus on “whoever was last to handle the drugs,” emphasizing proximity and causation rather than hierarchy or intent (Miller, 2021; Stepp, 2024).
New Jersey’s recent experience reflects this broader national trajectory. Between 2017 and the fourth quarter of 2025, the state’s Criminal Justice Data Dashboard reports 225 unique defendants charged under N.J.S.A. 2C:35-9, NJ’s DIH law, and related provisions, accounting for 262 charge filings10. For example, Atlantic County charged sixteen DIH offenses between 1988 and 2016 but filed thirteen additional charges by mid-2018 alone (Phillips, 2020). The state does not publish consolidated annual prosecution summaries, and an Open Public Requests Act (OPRA) request seeking centralized totals was denied as overbroad. Although charge-level data are publicly searchable, the absence of centralized reporting complicates independent evaluation of enforcement patterns and case outcomes under the statute.


Geographic Concentration, Racial Disparities, and Structural Context
Enforcement patterns must be understood within their geographic and demographic context. In 2024, 77% of New Jersey’s 11,295 naloxone administrations occurred in just 100 municipalities11. A similar pattern appears in arrest data: 77% of the state’s 20,291 drug-related arrests occurred within those same municipalities (ROIC, 2025). Yet only 62% of naloxone recipients and 50% of arrestees resided in those jurisdictions, indicating concentrated enforcement activity that extends beyond resident populations.
The municipalities most frequently appearing in overdose response and arrest data, including Newark, Camden, Jersey City, Trenton, Atlantic City, and Paterson, also experience significantly higher poverty rates than the statewide average12. These communities also have substantial Black and Hispanic populations. For example, Newark’s population is 45.7% Black and 37.6% Hispanic; Camden is 42.0% Black and 53.5% Hispanic; Paterson is 64.5% Hispanic; and Trenton is 41.3% Black and 46.4% Hispanic (U.S. Census Bureau, 2024). While demographic characteristics alone do not establish discriminatory intent, they provide critical context for understanding where enforcement activity is concentrated.
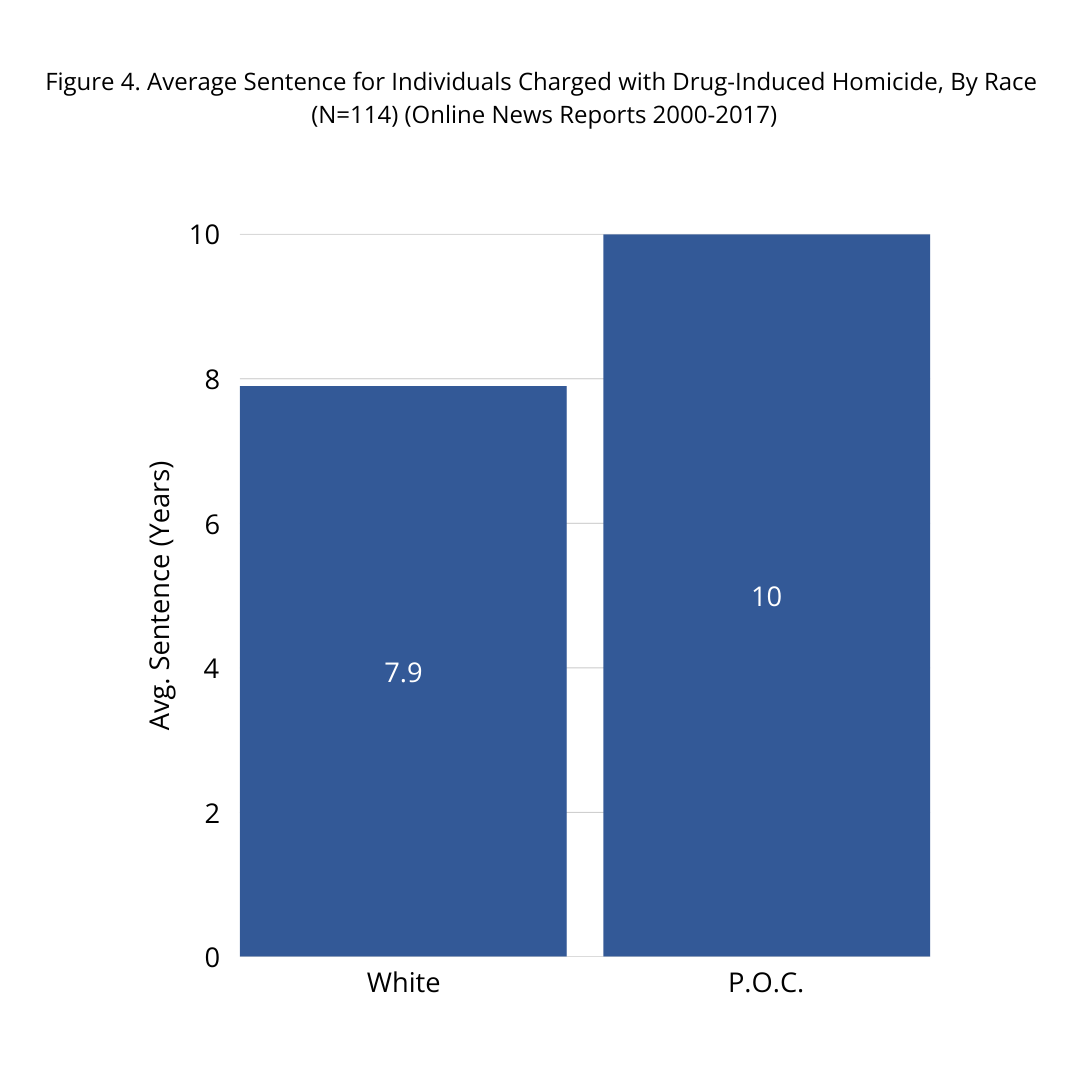
Statewide charge data further reflects racial disparity. Between 2017 and 2025, 51% of individuals charged under N.J.S.A. 2C:35-9 were categorized as Black, although Black residents comprise approximately 12–13% of the state’s overall population (New Jersey Office of Justice Data, 2026; U.S. Census Bureau, 2020). National analyses reinforce these concerns. A review of media-reported DIH cases between 2000 and 2017 found that people of color received average sentences of approximately 10 years, compared to 7.9 years for white defendants (Beletsky, 2019). Although based on reported cases rather than complete court records, this pattern aligns with longstanding racial disparities in sentencing across drug-related offenses.
These trends exist within a broader criminal legal system marked by profound racial imbalance. In New Jersey, Black residents are incarcerated at more than twelve times the rate of white residents and comprise roughly 60% of the state’s prison population despite representing approximately 15% of the overall population13. Evaluating strict liability drug-induced death prosecutions therefore requires situating enforcement within this larger structural landscape.
Public reporting confirms that strict liability drug-induced death charges have been filed across multiple New Jersey counties in recent years, including Burlington, Morris, Atlantic, Ocean, Bergen, Hunterdon, and Essex. Concentrations have shifted over time, with additional filings emerging in northern counties such as Bergen in 2024–2025. Several cases involve fentanyl or fentanyl-laced substances. While some cases include distribution-related allegations, publicly available records do not generally describe most defendants as operating large-scale trafficking enterprises.
County-level patterns reinforce the geographic overlap. Counties with the highest number of municipalities appearing in the top 100 naloxone administration and arrest lists include Camden, Ocean, Monmouth, Middlesex, and Burlington (ROIC, 2025). These counties overlap substantially with those identified as most impacted in the Statewide Drug Harm Index, which ranks Camden, Essex, Passaic, Atlantic, and Monmouth among the highest in drug-related harm based on overdose deaths, naloxone administrations, and drug submissions between 2019 and 202514. County rankings in the Statewide Drug Harm Index categories remain relatively stable over time, suggesting persistent geographic concentration of both drug-related harm and enforcement response.
ACLU-NJ. (2023). “Decarcerating New Jersey: A Transformative Vision of Justice.“
Prevention Implications
A review of publicly available case records in several strict liability prosecutions indicates that many defendants had prior contact with the municipal court system, including traffic offenses, regulatory violations, possession charges, and, in some instances, distribution-related offenses. While some defendants had prior drug distribution charges, publicly available records do not generally describe these cases as involving organized trafficking networks or large-scale narcotics enterprises. Instead, the records often reflect repeated lower-level system contact over many years prior to a fatal overdose event.
This recurring pattern raises a prevention-focused question: whether earlier points of contact within the municipal court and lower-level criminal system might represent opportunities for treatment referral, diversion, or harm reduction intervention. By the time a first-degree strict liability DIH charge is filed, the system response is post-fatal and incarceration-focused. Overdose prevention strategies, by contrast, are most effective before a death occurs. Any assessment of strict liability enforcement must therefore consider not only accountability after a fatality, but whether earlier public health interventions could reduce both overdose mortality and subsequent homicide-level prosecution.
Public Health Implications
A growing body of legal and public health scholarship raises concern that DIH prosecutions operate at cross-purposes with contemporary overdose prevention goals (Beletsky, 2019; Phillips, 2020; Stepp, 2024). While nearly all states have enacted overdose Good Samaritan laws to encourage individuals to seek emergency assistance, only a small number provide affirmative defenses within their DIH statutes for individuals who make a good faith effort to obtain medical help (Stepp, 2024). This structural gap creates tension between survival-oriented policy and punitive enforcement.

PEW. (2018). “More Imprisonment Does Not Reduce State Drug Problems.“
Importantly, existing empirical research has not demonstrated that heightened drug enforcement or homicide-style prosecution reduces overdose mortality. Legal scholarship reviewing drug-induced homicide statutes concludes that there is no empirical evidence linking DIH prosecutions to decreases in overdose deaths (Phillips, 2020). Similarly, a national analysis by the Pew Charitable Trusts found no statistically significant relationship between state drug imprisonment rates and levels of drug use, drug arrests, or drug overdose deaths, even after controlling for key demographic factors15. In short, states that incarcerate more individuals for drug offenses do not exhibit lower rates of overdose mortality. At the same time, involvement in the criminal legal system is associated with increased overdose vulnerability, disruption of treatment continuity, and reluctance to seek emergency assistance during overdose events (Phillips, 2020; Carroll et al., 2021; Stepp, 2024).
The contradiction is behavioral, not symbolic. Good Samaritan protections depend on credible assurances that seeking emergency assistance will not result in severe criminal exposure. When the same overdose event can also serve as the basis for a first-degree homicide investigation, that assurance weakens. Scholarship consistently finds that fear of arrest or prosecution can discourage emergency calls during drug-related crises (Phillips, 2020; Carroll et al., 2021). Beletsky (2019) argues that aggressive drug enforcement undermines overdose prevention by deterring help-seeking and reinforcing stigma.
Deterrence theory further complicates the rationale for strict liability expansion. Classic deterrence theory holds that certainty of enforcement, rather than severity of punishment, drives behavioral change. In the context of DIH prosecutions, where enforcement is uneven and highly case-specific, the threat of severe sentencing may have limited deterrent effect. Moreover, severe substance use disorder is widely recognized as a chronic medical condition characterized by compulsive use despite negative consequences. Individuals affected by severe SUD frequently discount long-term legal risks as a function of the illness itself. A policy framework that relies primarily on the threat of severe punishment to alter behavior risks fundamentally misconstrues the nature of substance use disorders (Beletsky, 2019).
As previously mentioned, Vermont provides a useful contrast. Its statute includes affirmative defense protections within its DIH framework for individuals who seek emergency assistance. Following implementation, the state reported modest declines in drug-related mortality during a period of high emergency response engagement (Miller, 2021). While causation cannot be established, the example illustrates that expansive help-seeking protections are not incompatible with active overdose response systems.
Racial equity concerns further intensify this tension. Scholarship has observed that DIH statutes may replicate longstanding disparities embedded within drug law enforcement and felony murder doctrine (Beletsky, 2019). Research indicates that these charges may be applied selectively and may produce sentencing disparities across racial groups (Beletsky, 2019). When homicide-level charges are brought in the context of substance use disorders and social use networks, the resulting harm extends beyond the courtroom, compounding community trauma rather than alleviating it.
NJ Monitor. (2025). “Governor Murphy Proposes Changes to Keep Technical Parole Violators Out of Prison.“
In addition to public health concerns, fiscal considerations warrant scrutiny. New Jersey spends approximately $74,750 annually to incarcerate one individual, more than ten times the average annual cost of parole supervision, highlighting the budgetary implications of carceral responses compared with community-based supervision16. In a resource-constrained environment, policymakers must consider whether long-term incarceration following a fatal overdose represents the most effective use of state funds compared to upstream investments in treatment access, harm reduction, and community-based intervention.
In addition to immediate fiscal costs, first-degree convictions carry long-term collateral consequences, including barriers to employment, housing, and professional licensure. In many drug-induced homicide prosecutions, defendants are themselves substance users, and these consequences may complicate recovery and reintegration.
Individuals released after incarceration also face significantly elevated overdose risk during the reentry period, a phenomenon widely documented in public health literature. These downstream effects warrant consideration when evaluating whether strict liability prosecution advances long-term prevention objectives.
The issue is not whether overdose deaths warrant accountability. Rather, it is whether strict liability homicide prosecutions, often applied to individuals who are themselves substance users, advance prevention goals or inadvertently contribute to continued cycles of harm after a fatality has occurred.
Ultimately, the policy balance reflects a choice. States can invest in punishment after death, or they can invest in prevention before it occurs. When those objectives diverge, prevention, not prosecution, should take precedence. If drug-related death is a public health emergency, the law must act like it.
Conclusion
DIH statutes were born from a supply-side enforcement philosophy that presumed severe punishment would deter distribution and protect communities. Decades later, amid a fentanyl analogue-driven overdose crisis, that premise warrants renewed scrutiny. Scientific understanding of substance use disorders has evolved. Public health responses have evolved. Harm reduction strategies have demonstrated effectiveness. Yet strict liability homicide frameworks remain anchored in an earlier punitive paradigm, despite a lack of demonstrated evidence that such prosecutions reduce overdose mortality.
Both national and New Jersey data demonstrate that individuals most frequently prosecuted under these statutes are not large-scale trafficking “kingpins,” but often friends, intimate partners, or family members; many struggling with substance use themselves. When earlier system contact fails to connect individuals to treatment or harm reduction services, the homicide prosecution that follows is necessarily reactive. By the time the statute is invoked, prevention has already failed.
The existing research does not show that heightened punishment reduces overdose deaths. It does, however, document concentrated enforcement in economically distressed communities, racial disparities in charging and sentencing, and legal structures that may discourage emergency help-seeking during overdose events. In this context, strict liability prosecution risk undermining the very public health goals states have simultaneously embraced.
DIH prosecutions may offer the appearance of accountability in the aftermath of tragedy. But appearance is not the same as effectiveness. If overdose is a public health emergency, the central question is not whether punishment feels proportionate; it is whether it saves lives. Where prevention and prosecution diverge, prevention must prevail. The measure of drug policy is not how forcefully it responds after death, but how effectively it prevents the next one.
REFERENCES
ACLU-NJ. (2021). New Jersey Racial and Ethnic Disparities in Prisons are Worst in the Nation. https://www.aclu-nj.org/press-releases/report-new-jersey-racial-and-ethnic-disparities-prisons-are-worst-nation/
ACLU-NJ. (2023). New Jersey prisons continue to show the highest rate of racial disparity nationwide. https://www.aclu-nj.org/publications/decarcerating-new-jersey-transformative-vision-justice/
Beletsky, L. (2019). America’s favorite antidote: Drug-induced homicide in the age of the overdose crisis. Utah Law Review, 2019(4), 833–900.
Carroll, J. J., Ostrach, B., Wilson, L., & Morales, M. (2021). Drug-induced homicide laws may exacerbate opioid-related harms: An example from rural North Carolina. International Journal of Drug Policy, 97, 103367. https://doi.org/10.1016/j.drugpo.2021.103367
County Health Rankings & Roadmaps. (2024). Good Samaritan drug overdose laws. https://www.countyhealthrankings.org/strategies-and-solutions/what-works-for-health/strategies/good-samaritan-drug-overdose-laws
DiFilippo, D. (2025, January 14). Governor Murphy proposes changes to keep technical parole violators out of prison. New Jersey Monitor. https://newjerseymonitor.com/2025/01/14/governor-murphy-proposes-changes-to-keep-technical-parole-violators-out-of-prison/
Jakubowski, A., Kunins, H. V., Huxley-Reicher, Z., & Siegler, A. (2018). Knowledge of the 911 Good Samaritan law and 911-calling behavior of overdose witnesses. Substance Abuse, 39(2), 233–238. https://doi.org/10.1080/08897077.2017.1387213
Miller, J. M. (2021). Save a friend’s life or risk your freedom: The dilemma too many people face when witnessing an overdose. Journal of Civil Rights and Economic Development, 34(3), 351–398.
New Jersey Office of Justice Data. (2026). Criminal justice data dashboard. https://www.njoag.gov/justicedata/
New Jersey Regional Operations Intelligence Center (ROIC), Drug Monitoring & Analysis Unit. (2025, April 7). Top 100 municipalities: Naloxone administrations & drug arrests (January 1, 2024 – December 31, 2024) (ROIC202503-08099D) [Report].
New Jersey Regional Operations Intelligence Center (ROIC), Drug Monitoring & Analysis Unit. (2026, February 20). Statewide drug harm index (January 1, 2019 – December 31, 2025) (ROIC202602-03375D) [Report].
Office of the Attorney General of New Jersey. (2013). Directive implementing the Overdose Prevention Act. https://nj.gov/oag/newsreleases13/pr20130702a.html
Pamplin, J. R., Rouhani, S., Davis, C. S., King, C., & Townsend, T. N. (2023). Persistent criminalization and structural racism in U.S. drug policy: The case of overdose Good Samaritan laws. American Journal of Public Health, 113(S1), S43–S48.
Phillips, K. S. (2020). From overdose to crime scene: The incompatibility of drug-induced homicide statutes with due process. Duke Law Journal, 70(3), 659–704.
Pew Charitable Trusts. (2018). More imprisonment does not reduce state drug problems: Data show no relationship between prison terms and drug misuse. https://www.pew.org/en/research-and-analysis/issue-briefs/2018/03/more-imprisonment-does-not-reduce-state-drug-problems
Stepp, S. N. (2024). Drug-induced homicide: A harsh weapon in the war on drugs. Boston College Law Review, 65(8), 2937–2972.
U.S. Census Bureau. (2024). QuickFacts: Newark city, New Jersey. https://www.census.gov/quickfacts/newarkcitynewjersey
U.S. Census Bureau. (2024). QuickFacts: Camden city, New Jersey. https://www.census.gov/quickfacts/camdencitynewjersey
U.S. Census Bureau. (2024). QuickFacts: Paterson city, New Jersey. https://www.census.gov/quickfacts/patersoncitynewjersey
U.S. Census Bureau. (2024). QuickFacts: Trenton city, New Jersey. https://www.census.gov/quickfacts/trentoncitynewjersey
U.S. Census Bureau. (2024). QuickFacts: Atlantic City city, New Jersey. https://www.census.gov/quickfacts/atlanticcitycitynewjersey
U.S. Census Bureau. (2024). QuickFacts: New Jersey. https://www.census.gov/quickfacts/NJ
- [↩]Beletsky, L. (2019). America’s favorite antidote: Drug-induced homicide in the age of the overdose crisis. Utah Law Review, 2019(4), 833–900.
- [↩]Stepp, S. N. (2024). Drug-induced homicide: A harsh weapon in the war on drugs. Boston College Law Review, 65(8), 2937–2972.
- [↩]Miller, J. M. (2021). Save a friend’s life or risk your freedom: The dilemma too many people face when witnessing an overdose. Journal of Civil Rights and Economic Development, 34(3), 351–398.
- [↩]Office of the Attorney General of New Jersey. (2013). Directive implementing the Overdose Prevention Act. https://nj.gov/oag/newsreleases13/pr20130702a.html
- [↩]Phillips, K. S. (2020). From overdose to crime scene: The incompatibility of drug-induced homicide statutes with due process. Duke Law Journal, 70(3), 659–704.
- [↩]Carroll, J. J., Ostrach, B., Wilson, L., & Morales, M. (2021). Drug-induced homicide laws may exacerbate opioid-related harms: An example from rural North Carolina. International Journal of Drug Policy, 97, 103367. https://doi.org/10.1016/j.drugpo.2021.103367
- [↩]Pamplin, J. R., Rouhani, S., Davis, C. S., King, C., & Townsend, T. N. (2023). Persistent criminalization and structural racism in U.S. drug policy: The case of overdose Good Samaritan laws. American Journal of Public Health, 113(S1), S43–S48.
- [↩]County Health Rankings & Roadmaps. (2024). Good Samaritan drug overdose laws. https://www.countyhealthrankings.org/strategies-and-solutions/what-works-for-health/strategies/good-samaritan-drug-overdose-laws
- [↩]Jakubowski, A., Kunins, H. V., Huxley-Reicher, Z., & Siegler, A. (2018). Knowledge of the 911 Good Samaritan law and 911-calling behavior of overdose witnesses. Substance Abuse, 39(2), 233–238. https://doi.org/10.1080/08897077.2017.1387213
- [↩]New Jersey Office of Justice Data. (2026). Criminal justice data dashboard. https://www.njoag.gov/justicedata/
- [↩]New Jersey Regional Operations Intelligence Center (ROIC), Drug Monitoring & Analysis Unit. (2025, April 7). Top 100 municipalities: Naloxone administrations & drug arrests (January 1, 2024 – December 31, 2024) (ROIC202503-08099D) [Report].
- [↩]U.S. Census Bureau. (2024). QuickFacts: Newark city, New Jersey. https://www.census.gov/quickfacts/newarkcitynewjersey
- [↩]ACLU-NJ. (2021). New Jersey Racial and Ethnic Disparities in Prisons are Worst in the Nation. https://www.aclu-nj.org/press-releases/report-new-jersey-racial-and-ethnic-disparities-prisons-are-worst-nation/
- [↩]New Jersey Regional Operations Intelligence Center (ROIC), Drug Monitoring & Analysis Unit. (2026, February 20). Statewide drug harm index (January 1, 2019 – December 31, 2025) (ROIC202602-03375D) [Report].
- [↩]Pew Charitable Trusts. (2018). More imprisonment does not reduce state drug problems: Data show no relationship between prison terms and drug misuse. https://www.pew.org/en/research-and-analysis/issue-briefs/2018/03/more-imprisonment-does-not-reduce-state-drug-problems
- [↩]DiFilippo, D. (2025, January 14). Governor Murphy proposes changes to keep technical parole violators out of prison. New Jersey Monitor. https://newjerseymonitor.com/2025/01/14/governor-murphy-proposes-changes-to-keep-technical-parole-violators-out-of-prison/